Why worry about a cure for heart attack and stroke when you can prevent it altogether?
This is a follow-up article to an initial post on how I reversed 20 years of arterial plaque.
How a heart attack happens
Let’s look at some images first.
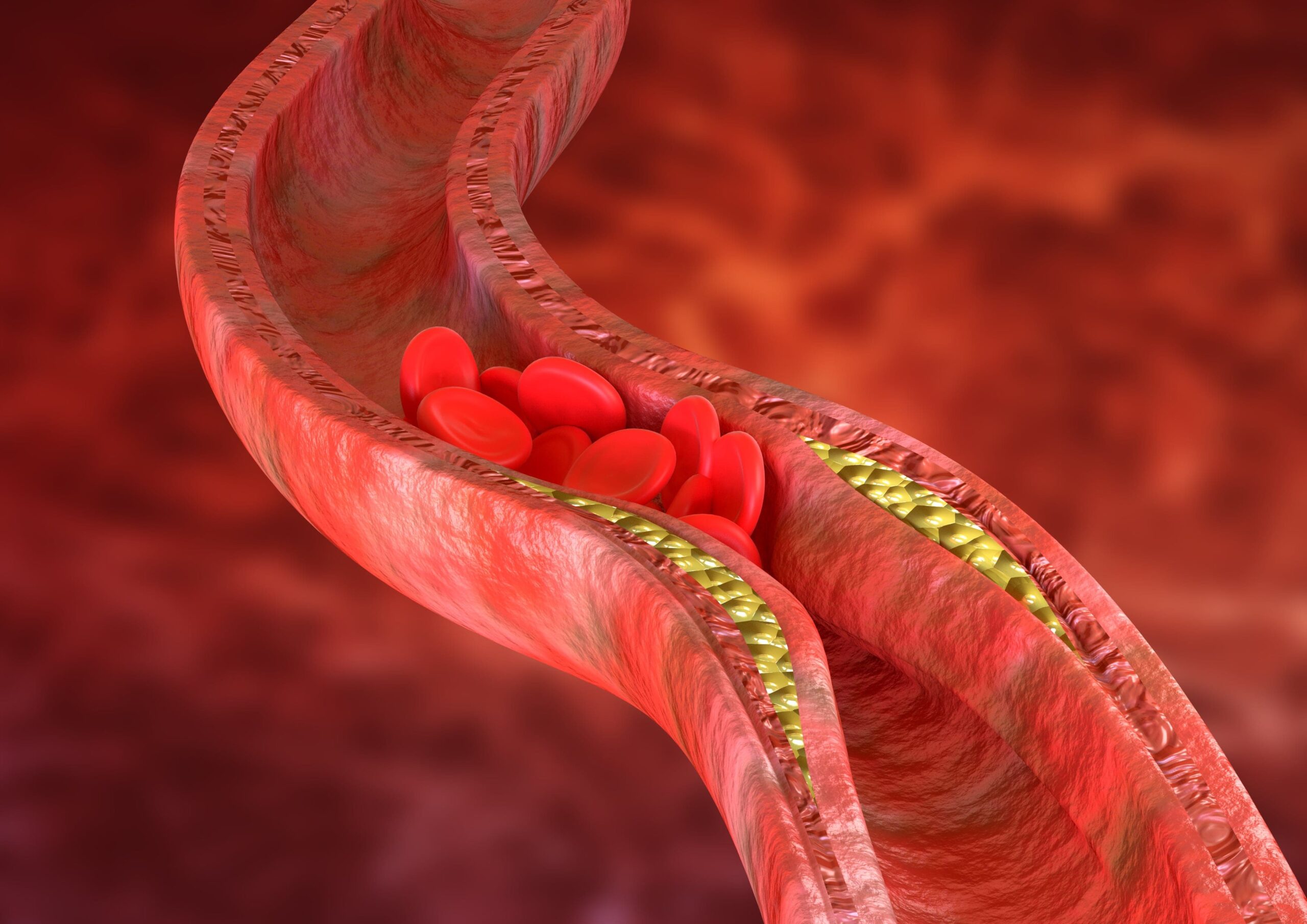
Here is a normal artery. The lumen is the hole where blood flows. On heart attacks and strokes, we’re worried about 2 layers: the intima and the media.
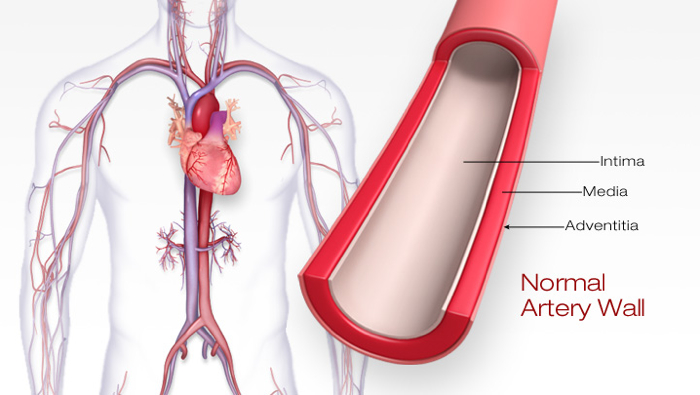
The intima is the inner lining that keeps the blood from clotting and performs other metabolic actions. The media is the muscle layer that provides structure. If you didn’t have that muscle layer, the inner layer would just burst apart. This happens when LDL cholesterol goes into the intima-media space.
Here are a few things to know about plaque.
One, plaque doesn’t fill the inside of the lumen like hair clogging a drain.
Two, plaque leaking into the bloodstream may not be enough to block the lumen.
Three, you don’t get a heart attack from slow blockage of that hole—you get it from fast blockage.
How does fast blockage occur?
The problem lies in “hot” or inflamed plaque that could be released into the bloodstream. As LDL cholesterol gets lodged into the intima-media space, it grows into a plaque, but the intima keeps plaque away from the bloodstream.
However, CV inflammation could turn plaque into a “hot” plaque. And if this “hot” or inflamed plaque leaks into the bloodstream, it could form a clot.
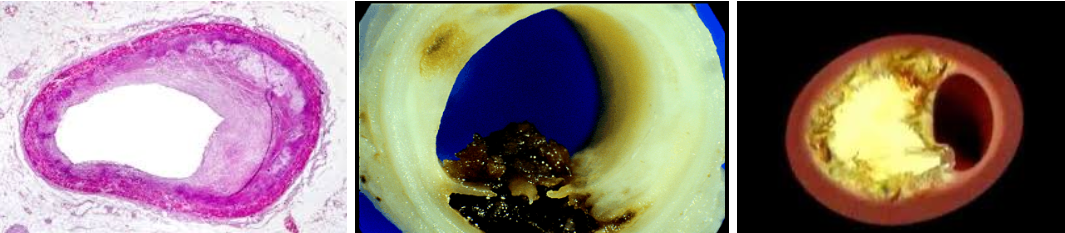
See the black spot in the middle image above. That’s a clot. It broke off, went to the heart, caused a heart attack, and killed this patient.
Arterial age and CIMT
While stress tests are common tests, they won’t show a true positive result until the patient has over 50% blockage.
Just look at broadcast journalist Tim Russert; he had a normal stress test 3 months before he succumbed to a heart attack in 2008. At post-mortem, Russert’s arteries looked more like a teenager’s face with lots of pimples and bumps than a clogged drain.
That’s why I prefer that my patients get a carotid intima-media thickness (CIMT) scan over a stress test.
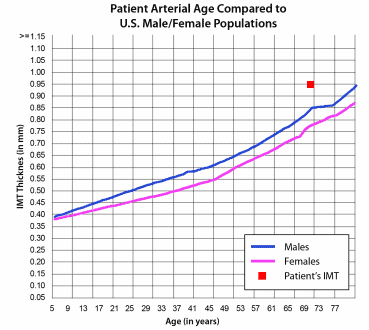
On the right is a sample nomogram you’ll see in a CIMT test report. The 2 lines show what should be the normal CIMT by age for men and women. Using your CIMT value, you can look where you are positioned in the nomogram, and that will give you your arterial age.
There is a lot of argument, though, about whether we should use the concept of arterial age. CIMT and arterial age reflect the ingress or egress of LDL cholesterol into the intima-media space, so I don’t see us getting away from the concept of arterial age anytime soon.
My CIMT test results
I was a poster boy for heart attack and stroke prevention. I had a great diet. I had a great exercise regimen. My BMI had always been less than 25.
So when I went through my first CIMT scan, I expected to do a victory lap. Instead, what I found out was that I had 73-year-old arteries at age 57! That’s way older than my actual age when I underwent my first CIMT scan in February 2015.
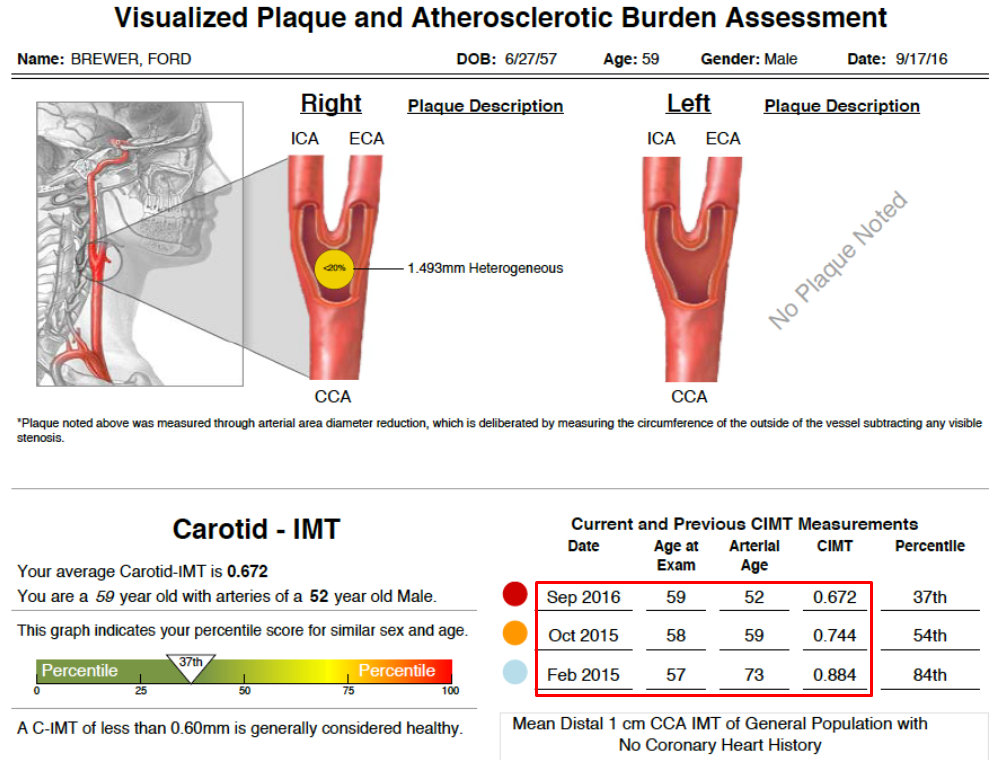
It’s a great thing that I improved after my first CIMT scan—I went from 73 to 59 to 52 in terms of arterial age. In September 2016, my arterial age drastically dropped from that of the 73-year-old to that of a 52-year-old.
So whether you believe in arterial age estimation, it is crystal clear that I had massive egress of LDL cholesterol out of the space between my intima and media layers.
My CIMT values are another number to look at. My average CIMT in 2016 was 0.67 mm. If you go back to my original CIMT, my average was 0.88 mm. Again, it’s clear that I pulled a lot of LDL cholesterol out of my intima-media space.
How I reversed my arterial age
You may ask: This guy is doing the right stuff in terms of heart attack and stroke in the first place, but why did he still have this kind of arteries?
It’s genetics. I have 9p21, a gene originally thought to be a cancer gene but later was found out to be a heart attack gene. Then we found out that I also have a diabetes gene, something that puts all these things together.
How did I dramatically improved my arterial health?
I made further changes to my lifestyle. I lost another 5 lbs. I added some supplements, like niacin. I also started statin for inflammation. I also changed my blood pressure medicine from Losartan (an ARB) to Ramipril (an ACE inhibitor). I started taking combinations of pioglitazone and metformin. I continued to manage my insulin resistance.
Here’s something else you need to know about insulin resistance. Over half of us have insulin resistance by the time we reach the age of 60. By the time we are 65, 25% of us are full-blown diabetics. That’s the definition by ADA (American Diabetes Association), which is an extremely conservative definition.
Remember this: If you’re insulin-resistant, you’re already doing tons of damage to your arteries in your heart, kidneys, eyes, other tissues before you get a full-blown diagnosis of diabetes. So don’t wait until you get full-blow diabetes before you act.
If you found this article helpful and want to start taking steps toward reversing your chronic disease, Dr. Brewer and the PrevMed staff are ready to serve you no matter where you’re located.
To find out more, schedule a consult here: prevmedhealth.com