What are the things that can cause heart attacks and strokes?
This should be an excellent discussion because once we know what causes cardiovascular (CV) diseases, then we can prevent them. Things may be difficult but not nearly as much as undergoing a surgery (like a coronary artery bypass) or worse, decades of disability as often seen with people who had a stroke, with heart failure, or have dementia.
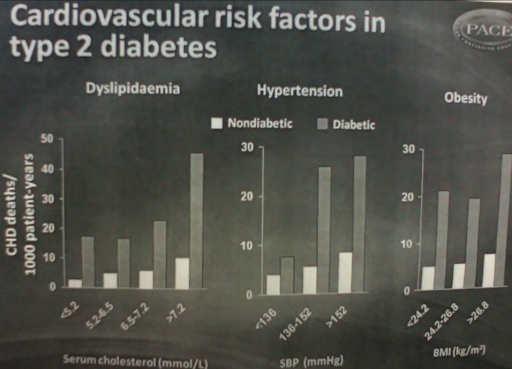
Look at the slide above. This is from a study titled “Diabetes and Long-Term Risk of Mortality From Coronary and Other Causes in Middle-Aged Swedish Men: A general population study” (Adlerberth et al., 1998).
It compares the number of cardiovascular deaths between nondiabetics and people with diabetes. It looks at several risk factors simultaneously:
- Dyslipidemia: Bad lipids or fats in the blood, which can be seen in a cholesterol panel. Increasing serum cholesterol has a correlation with higher CVdeaths.
- Hypertension: High SBP (systolic blood pressure) is an increased risk factor for heart attack and stroke. More CV deaths appear to occur at higher SBP ranges.
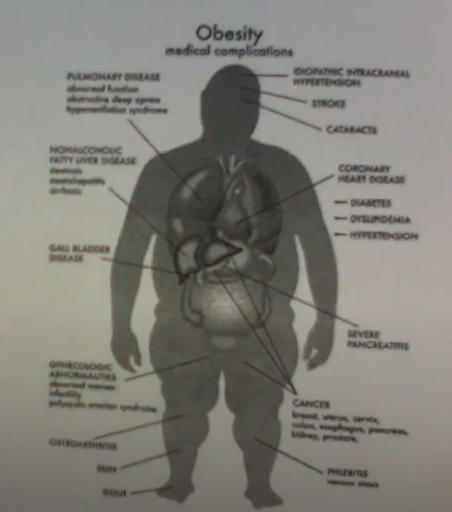
- Body mass index (BMI): High BMI or obesity deserves to be mentioned, as an obese person has increased risk for heart disease, diabetes, dyslipidemia, and high blood pressure.
In these 3 risk categories, there is a higher probability of CV deaths among diabetics than nondiabetics, showing that diabetes itself is also a significant CV risk.
This video comprehensively shows the connections between various CV risk factors.
Diabetes and prediabetes as risk factors
Diabetes is not only putting people vulnerable to CV disease. Nowadays, with COVID-19, one pattern we’re seeing is the increased risk caused by pre-existing conditions, which include diabetes and prediabetes.
Why is COVID-19 dangerous for diabetics and prediabetics? This may have to do with fluctuating blood glucose levels and diabetes complications.
While recent focus has been on bats, cruise ships, hydroxychloroquine, vitamin C, mass testing quandaries, personal protective equipment, among other things, more people are still dying because of CV diseases than COVID-19. That’s how lethal heart attacks and strokes are.
And the leading cause of heart attack and stroke? Diabetes and prediabetes.
In fact, prior to COVID-19, we have all been dealing with the longer, bigger, more lethal diabetes/prediabetes pandemic.
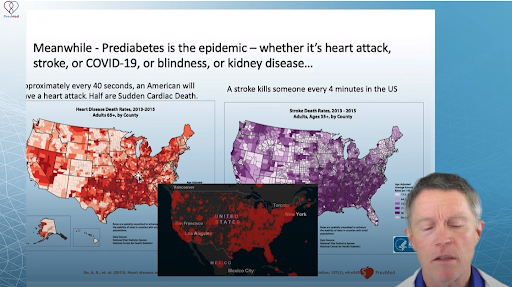
Shown above are 3 maps. The left is a map of heart disease death rates in the US. On the right is a map of stroke death rates in the US. In the middle is a map for COVID-19 deaths.
What’s the common factor in all 3 maps?
Diabetes/prediabetes is the underlying risk, with heart attacks, strokes, and COVID-19 as the grim reapers causing the eventual death. That’s why diabetes and prediabetes are serious issues (if not more serious) like COVID-19.
Diabetes vs. prediabetes
But why give weight to prediabetes?
It’s unfortunate that many people have this motion that prediabetes is just “a touch of sugar,” that they won’t have to worry unless they have full-blown diabetes.
That’s not true at all. For instance, many people already have eye diseases or retinopathy, which leads to diabetes-associated blindness, even before they are diagnosed as full-blown diabetic.
An artery with a plaque that’s been inflamed for years could release hot plaque into the bloodstream. Hot plaque could cause a clot. If the clot is big enough and it goes to the heart, it causes a heart attack. If it’s big enough and it goes to the brain, that’s called a stroke.
What causes this plaque to get laid down and burned in the first place?
Having hours after hours of high blood sugar. Such a thing happens not only with diabetics but also with prediabetics. That’s the primary danger of ignoring prediabetes and only starting to act when diagnosed with full-blown diabetes.
Still, you may think of prediabetes as the same disease as diabetes, perhaps a tad lower.
But if you’re prediabetic, that simply means you haven’t met yet the lab testing cut-off to be considered a diabetic, but you’re already in the same disease process. (We’ll explain this in the next section.)
Prediabetes vs. insulin resistance vs. metabolic syndrome
We always mention insulin resistance and prediabetes in our YouTube videos but rarely mention metabolic syndrome.
These terms—prediabetes, insulin resistance, and metabolic syndrome—are used interchangeably, and there’s a boatload of confusion in this area. Their definitions, though, point to the same process.
Prediabetes
Prediabetes is the disease model.
But before we tackle prediabetes, let’s talk about diabetes again. We know diabetes is the inability to metabolize sugar properly. So let’s say for now that prediabetes (prefix “pre” means “before”) is the stage of the disease before full-blown diabetes.
There are different ways of defining the transition from normal glucose levels to prediabetes to diabetes. For example, this is the diagnostic criteria from Diabetes.co.uk. Prediabetes is defined as having:
- a fasting plasma glucose between 5.5-7.0 mmol/L;
- hemoglobin A1c (hbA1c) between 42-47mmol/L or 6.0-6.4%; or
- OGTT (oral glucose tolerance test) between 7.8-11.1 mmol/L.
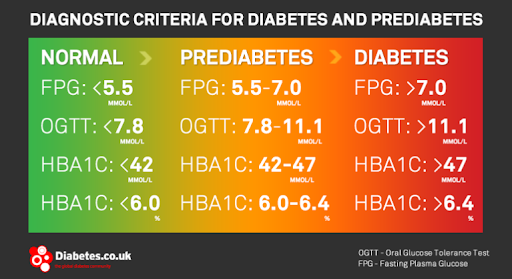
These criteria show that there is a progression from having totally perfect glucose metabolism to having full-blown diabetes.
However, there are debates on this topic, like, where do we split diabetes and prediabetes, or prediabetes and normal glucose level?
While the multiple ways for testing blood glucose levels (like fasting blood glucose, OGTT, and hbA1c) help settle the debates, things are still unclear. There are confusing variations in terms of the unit of measurement used (English vs. metric) as well as the cut points, depending on who you are referring to.
Here’s an example. If hbA1c is 6.4%, the person is still prediabetic. Many people would still assume this to be relatively “safer” than being a diabetic. But when hbA1c is 6.5%, the person is already diabetic. But is 0.1% such a sizeable difference? Should the person not be concerned with 6.4% but be worried about 6.5%?
Major organizations, like WHO (World Health Organization), ADA (American Diabetes Association), and IEC (International Expert Committee on Diabetes) also offer varying ranges for defining prediabetes.
- For fasting blood glucose, WHO and ADA have the same range for prediabetes (100-125 mg/dL); IEC doesn’t have any. If you check the image above from Diabetes.co.uk, mmol/L is used as the unit for fasting blood glucose measurement, which fuels further confusion.
- For hbA1c, ADA and IEC differ significantly on hbA1c. ADA’s minimum limit is down to 5.7%; IEC says one doesn’t have prediabetes until hBA1c is 6.0. Diabetes.co.uk concurs with IEC, while WHO doesn’t have any range for hbA1c.
| Test |
WHO* |
ADA* | IEC* |
| Fasting Glucose | 100 – 125 mg/dL | 100 – 125 mg/dL | – |
| 2-hour Glucose | 140 – 199 mg/dL | 100 – 125 mg/dL | – |
| HbA1c | – | 5.7 – 6.4% | 6.0 – 6.4% |
If you talk to experts, they say a different thing too. Jenny Ruhl, the author of “Blood Sugar 101” says you’re already getting damage any time your hbA1c crosses the 5% threshold. There are certain studies that support this premise.
So with all these different references, it’s tough to know exactly how much damage is enough before we acknowledge that there is a problem.
So don’t let the “pre” in prediabetes fool you. Don’t assume that it’s just a stage prior to full-blown diabetes. Prediabetes is already a serious health condition on its own. Like diabetes, it also leads to heart attack and stroke.
Insulin resistance
Insulin resistance is a biochemical definition, describing what’s going on biochemically. It means the body is not responding effectively to insulin.
This image below illustrates insulin resistance (from “Adipokines Mediate Inflammation and Insulin Resistance;” Kwon and Pessin, 2013). Insulin receptors found in either liver or muscle cells are involved in this biochemical process.
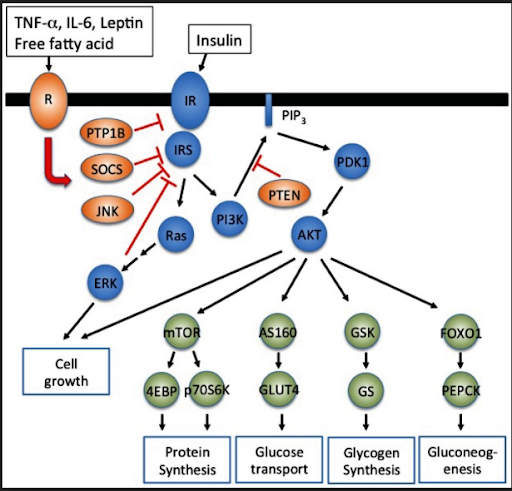
When blood sugar gets too high (over 125 mg/dL), there are activities that start happening biochemically when insulin is released. When insulin is released, this activates insulin receptors to pull sugar out of the blood into the liver or muscle. This is done to decrease blood sugar.
However, if insulin receptors become less responsive or less sensitive to insulin, there would be too much glucose or too much in the blood. This is bad as this drives plaque growth or impairs many metabolic processes.
Metabolic syndrome
The third concept, metabolic syndrome, is a clinical model.
Merriam-Webster defines “syndrome” as “a group of signs and symptoms that occur together and characterize a particular abnormality or condition.” It is basically a cluster of symptoms. Doctors sometimes are aware of the symptoms, sometimes they don’t, so they just bunch them under a syndrome.
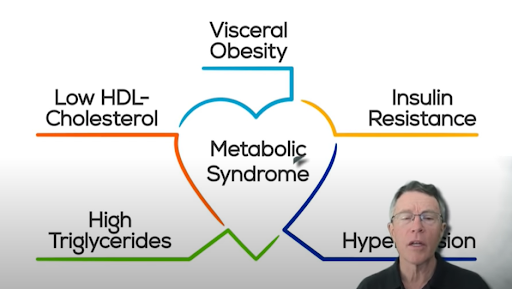
What is metabolic syndrome then? The image above probably is the most simple description of metabolic syndrome.
So as you can see, apart from insulin resistance, there are also visceral obesity, low HDL cholesterol, high triglycerides, and high blood pressure characterizing metabolic syndrome. Doctors have observed these conditions for a long time, suspected it to be just insulin resistance, then they bunched these symptoms together under “metabolic syndrome.”
To add to the confusion, different organizations also define metabolic syndrome differently.
Just look at the table below, taken from an article titled “The Prevalence of Metabolic Syndrome According to Various Definitions and Hypertriglyceridemic-Waist in Malaysian Adults” (Zainudin et al., 2011).
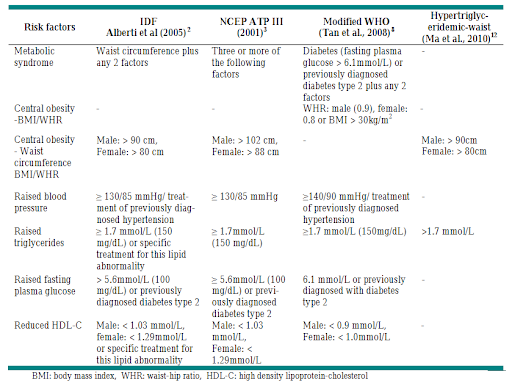
IDF looks at waist circumference plus 2 other factors. For NCEP ATP III, waist circumference is unnecessary. As long as 3 or more of the remaining factors are met, the person can be classified to have metabolic syndrome.
Here’s another way to look at metabolic syndrome: Excess fats around the waist are considered a metabolic syndrome component.
Not all people who have excess fats, though, have high blood pressure. On the other hand, a skinny person who appears to be fit and without abdominal fats may have high blood pressure.
Doctors see the syndrome components, so defining metabolic syndrome is not that straightforward.
That’s why we don’t use the term “metabolic syndrome” that much here in PrevMed. In our videos, you’ll often hear us mention prediabetes or insulin resistance.
Prediabetes tests
We have now established that arterial plaque can cause heart attack (the number one killer), stroke (the number one disabler), dementia (rapidly becoming the number one disabler as well), plus some other conditions like blindness, kidney disease, and erectile dysfunction.
We also have established by now that elevated blood sugar, prediabetes, and/or diabetes can cause plaque growth.
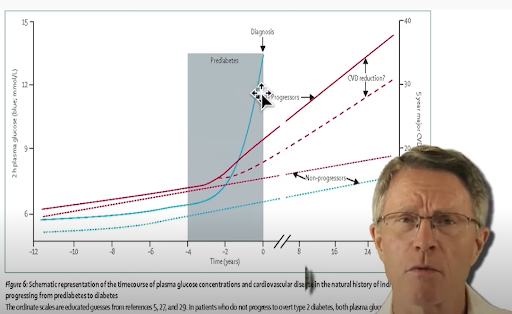
This graph above shows that the higher the blood sugar levels, the faster people develop plaque. But what’s interesting and frustrating at the same time is that only a few of us know what’s going on with our blood sugar levels and our ability to metabolize carbs.
What’s even more tragic is that testing to learn about our bodies is not that difficult or expensive to do.
It’s estimated that over 70% of people with plaque have insulin resistance. That’s actually a gross underestimate, and it’s because we’re not diagnosing insulin resistance that well. It’s diagnosed based only on hbA1c and fasting blood glucose.
HbA1c alone can miss up to half of patients with insulin resistance. That’s why it shouldn’t be used alone. Unfortunately, that’s the standard of medicine today.
Good thing, there are more definitive ways to test. Two of them are OGTT (oral glucose tolerance test) and Kraft insulin survey.
With OGTT and Kraft insulin survey, we can now properly diagnose the other 30% to show that they have carb metabolism problems. So anyone with known plaques is recommended to be tested with at least an OGTT or preferably with a Kraft insulin survey.
OGTT
During an OGTT, you would be tested for fasting blood glucose then given a 75-g of glucose drink. After this, your glucose levels are to be tested after half an hour, an hour, and 2 hours.
If you have a one-hour OGTT of 125 mg/dL or more, you’ve got 13 times the risk of full-blown diabetes over the next 7 to 8 years. A 2-hour value that’s between 120 to 139 is common among 50- and 60-year-olds.
If you’re among this population, this means you got about a third of your beta cells in your pancreas that are still functional. Your beta cells may put out significant insulin to bring down your blood glucose, but that is not providing the expected effect.
In other words, your insulin receptors in your liver and muscle cells are resistant to insulin.
Kraft insulin survey
The Kraft insulin survey was developed by Robert Kraft.
In this test, you would be tested for fasting blood glucose then given a 100-g of glucose drink. Then you are tested for glucose levels after half an hour, 1 hour, 2 hours, 3 hours, and 4 hours.
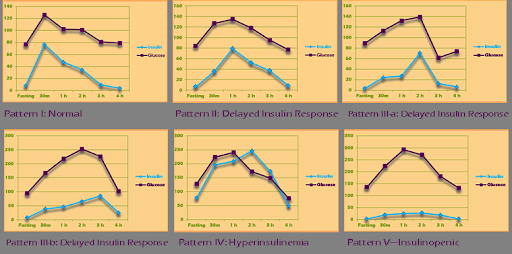
The key difference of Kraft insulin survey from OGTT is that insulin levels are also taken at these intervals. The insulin testing would help you more in telling whether you have normal insulin production, you have a normal or delayed insulin response, or you’re producing lots of insulin but you’re resistant to it.
Your results would be plotted to look like one of the prediabetes profiles shown below.
If you want to know more about prediabetes and these 2 prediabetes tests, check out our insulin resistance course. Even better, you can get tested for OGTT and insulin survey tests by enrolling in our Insulin Resistance/CV Inflammation webinar.
How common is prediabetes?
We’ve covered prediabetes tests. We’ve differentiated diabetes, prediabetes, insulin resistance, and metabolic syndrome.
But who cares about prediabetes?
For one, the CDC (Centers for Disease Control and Prevention) do care.
CDC says that among 84 million Americans out there, a third of those have prediabetes. Worse, 90% of prediabetics don’t know that they have the condition.
However, the University of California, Los Angeles (UCLA) reported a higher figure—55% got prediabetes. This study, however, was only based on fasting blood glucose and hbA1c tests. If UCLA researchers considered the more definitive OGTT and Kraft insulin survey tests, the number could have gone up to as high as 70%!
Worse, prediabetes is not a disease that we have to wait until the age of 50+ to hit us. Over half of us already have prediabetes by the age of 30!
Upon closer inspection, prediabetes already presents significant risks for heart attack and stroke.
Therefore, we should care about prediabetes and not wait until we have full-blown diabetes.
If you are insulin-resistant, glucose already remains in your blood at dangerously high levels. If prediabetes isn’t addressed promptly, this could lead not only to full-blown diabetes but also to chronic inflammation, heart attack, stroke, eye diseases, dementia, erectile dysfunction, kidney failure, and severe COVID-19.
These deadly conditions should be enough to convince you and other people that prediabetes is already a serious matter.
My name is Ford Brewer. My team and I work to prevent heart attack, stroke, cancer, and dementia. Our goal is to help you understand how to prevent major killers and disablers. Most of them are driven by the process of cardiovascular inflammation.
If you want to know more about the science of preventive medicine or you have questions about certain aspects of your health, check out our webinars, membership programs, and online courses.
If you’d like to learn about the basics of heart attack & stroke prevention for free, complete this form, and get access to our CV inflammation course. If you’re interested in how we can help you, check out our services page.