There’s been a lot of debate about niacin over the past decade. We’ll cover that topic in this post, describe niacin and its various forms, and the 2 studies that drove certain people to think niacin doesn’t work.
What is niacin?
Niacin or vitamin B3 is a water-soluble vitamin. It is naturally present in many foods, added to some food products, and available as a supplement.
Niacin is the generic name for various vitamin B3 forms, like nicotinic acid, nicotinamide, and nicotinamide riboside.
Nicotinic acid: Did you know that the term “niacin” is derived from “nicotinic acid vitamin”? So when talking about niacin, we usually refer to nicotinic acid. Nicotinic acid was first synthesized in 1800, but it wasn’t until 1937 that its chemical structure was discovered. Nicotinic acid and nicotinamide are the most common forms of dietary niacin.
Nicotinamide/niacinamide: Nicotinamide was discovered between 1935 and 1937. It is part of the WHO list of essential medicines. Compared to nicotinic acid, nicotinamide has the advantage of not causing skin flushing, a common side effect of niacin.
Nicotinamide riboside (NR): A relatively new form of niacin, NR was discovered in 1944. NR has unique properties that differentiate it from nicotinamide and nicotinic acid. It’s non-flush niacin like nicotinamide.
Niacin and metabolism
Inside the body, niacin is converted into NAD (nicotinamide adenine dinucleotide), a coenzyme, and a metabolically active form of niacin. NAD can be converted into NADP (nicotinamide adenine dinucleotide phosphate), also a coenzyme, and another active form of niacin.

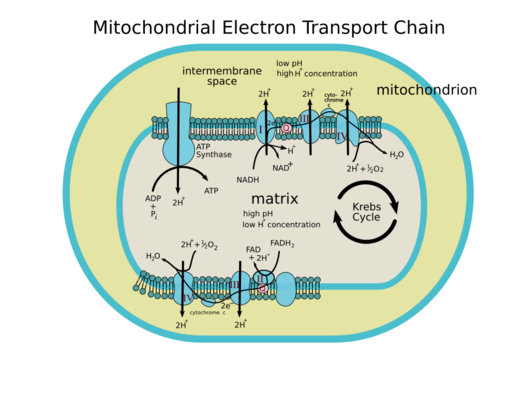
Above is a diagram of the mitochondrion. Below is a diagram of what happens inside the mitochondrion.
User:Rozzychan / CC BY-SA (https://creativecommons.org/licenses/by-sa/2.5)
You may recognize the TCA cycle (Krebs cycle) and oxidative phosphorylation, processes that involve NAD and NADP. This just shows that niacin is a major component in many areas of our metabolism. In fact, niacin is involved in over 450 metabolic processes.
Niacin and pellagra
Niacin (nicotinic acid to be exact) was synthesized in 1867, though it wasn’t used for any health purposes.
In 1937, American biochemist Conrad Arnold Elvehjem “rediscovered” niacin. He studied niacin’s effects against pellagra by withholding niacin in the diet of dogs. When the dogs developed a black tongue, he gave them niacin as treatment.
As niacin was found to cure and prevent pellagra, it was initially named the “P-P factor” (pellagra-preventive factor).
Pellagra is a multi-system vitamin B3 deficiency problem characterized by 4 Ds (diarrhea, dermatitis, dementia, and death) (Hegyi, 2004).

Herbert L. Fred, MD; Hendrik A. van Dijk / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)
Does niacin really work?
What’s the big deal about niacin?
Apart from treating pellagra, niacin is both a medicine and supplement that’s been shown to have many positive effects (Houston, 2014).
Niacin was used for decades for cardiovascular (CV) risk prevention. It’s the only thing that can increase HDL cholesterol and decrease LDL cholesterol. It’s one of the few things that could improve lipoprotein(a) or Lp(a). It affects oxidation, inflammation, lipid levels, and CV risk.
Many studies showed that niacin helps until these 2 studies—HPS2-THRIVE and AIM-HIGH—came along.
HPS2-THRIVE
HPS2-THRIVE came out first.
It stands for “Heart Protection Study 2–Treatment of HDL to Reduce the Incidence of Vascular Events.”
The goal of this 4-year study was to look at the effects of the combination of extended-release niacin and laropiprant in subjects at risk of CV events. Merck (the manufacturer of the laropiprant) funded the trial. The findings were published in 2014 in NEJM (HPS2-THRIVE Collaborative Group, 2014).
Niacin increases HDL cholesterol and lowers LDL cholesterol. However, niacin (nicotinic acid to be exact) is notorious for a flushing side effect because of a so-called prostaglandin effect.
Prostaglandins are hormone-like substances produced by body tissues. The prostaglandin effect leads to vasodilation. When niacin causes arteries and capillaries in the skin to dilate, that causes the flushing as well as the itching.
Laropiprant is a chemical that stops niacin’s flush effects. It blocks prostaglandin receptors that niacin was hitting with that flush. So patients who took the niacin-laropiprant combination didn’t exhibit the flush.
Did the niacin-laropiprant combo work?
Yes, and no. Laropiprant removed niacin’s flush effect, but it also got rid of the positive aspects of niacin.
In the end, HPS2-THRIVE researchers saw no improvement in CV events in patients who took the niacin-laropiprant combo, which prompted the press (and even doctors) to claim that niacin doesn’t work.
AIM-HIGH
Then came the AIM-HIGH.
It’s short for “Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/HIGH Triglycerides: Impact on Global Health Outcomes.” Findings were first published in NEJM in 2011 (AIM-HIGH Investigators, 2011).
It’s designed as a secondary prevention trial. The subjects had CV disease. They were already treated with 40-80 mg simvastatin and 10 g ezetimibe daily. AIM-HIGH researchers looked at whether niacin could prevent CV conditions from worsening.
The AIM-HIGH trial was expected to show improvement, but it didn’t. Once again, the press came out saying that AIM-HIGH is another proof that niacin doesn’t work.
Then the AIM-HIGH researchers came out and gave clarifications. Even principal AIM-HIGH investigator Dr. William Boden said he was afraid people would interpret the results wrongly.
Misinterpreting the AIM-HIGH results
Here are a few things that made AIM-HIGH interpretation murky:
(1) I believe the patients were overmedicated and undermanaged in terms of lifestyle. To reach the aggressive goal of 40-80 mg/dL LDL cholesterol levels, all subjects were put on 40-80 mg of simvastatin and 10 g ezetimibe daily, plus doses of extended-release niacin that increased weekly from 500 mg to 2 g. The possible effect of statins on increasing HDL cholesterol further adds complications.
(2) Subjects who exhibited flushing at 1.5-2 g niacin range were then separated into the niacin and placebo groups. Researchers used immediate-release niacin as a matching placebo. But since immediate-release niacin causes a flush, it should be easy for a subject to know whether he’s on placebo. To mask the flush, subjects in the placebo group were only given 50 g immediate-release niacin, a tiny dose.
(3) The original intent of AIM-HIGH was to study around 4,000 people for around 7 years, and researchers wanted to accrue 800 events. Endpoints in this study are heart attack, stroke, CV hospitalization, or death. However, the study stopped in 36 months. To complicate the matter, the niacin group appeared to have more potential for ischemic stroke.
The bottom line: Anyone who says niacin didn’t work was ignoring tons of other studies that indicate the effectiveness of niacin. Dr. Boden said it’s premature to abandon niacin, and my credits to him for being open and honest about the challenges he worked through in this study.
Do I take niacin?
Niacin works, and I recommend it. I take 2 grams of niacin per day.
I occasionally get a flush. It’s not bad because I take an extended-release brand.
Moreover, many people have few problems with niacin. If you’re one of those people that experiences side effects, be glad to know that the problems associated with niacin can be easily overcome, like trying non-flush niacin versions.
If you found this article helpful and want to start taking steps toward reversing your chronic disease, Dr. Brewer and the PrevMed staff are ready to serve you no matter where you’re located.
To find out more, schedule a consult here: prevmedhealth.com
References
AIM-HIGH Investigators, Boden WE, Probstfield JL, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy [published correction appears in N Engl J Med. 2012 Jul 12;367(2):189]. N Engl J Med. 2011;365(24):2255-2267. doi:10.1056/NEJMoa1107579
Hegyi J, Schwartz RA, Hegyi V. Pellagra: dermatitis, dementia, and diarrhea. Int J Dermatol. 2004;43(1):1-5. doi:10.1111/j.1365-4632.2004.01959.x
Houston M, Pizzorno J. “Niacin Doesn’t Work and Is Harmful!” Proclaim the Headlines. Yet Another Highly Publicized Questionable Study to Discredit Integrative Medicine. Integr Med (Encinitas). 2014;13(5):8-11.
HPS2-THRIVE Collaborative Group, Landray MJ, Haynes R, et al. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371(3):203-212. doi:10.1056/NEJMoa1300955