Contrary to popular belief, being lean doesn’t always mean being healthy. On the other hand, obesity might cause different degrees of metabolic issues. If you find this confusing, don’t miss this blog, as it takes an in-depth look into fats and fat metabolism, according to diabetes expert Dr. Philipp Scherer.
Dr. Scherer is the Director of Touchstone Diabetes Center at the University of Texas-Southwest Medical Center. He’s won the Triple Crown for diabetes research and the Gerald Shulman’s Banting Lecture Award, which recognizes the lifetime contribution to the science of diabetes.
You can read more about him here:

Dr. Scherer points out that we think of the fat cell as just a simple sack with fat in it. And that’s where we store fatty acids between fasting episodes. His point is, “no, the fat cell is highly complex, it’s an endocrine cell, it releases hormones called adipokines. Leptin is the most commonly known of the group, and there are lipids and metabolites in it”.
What goes wrong in our adipose tissue when we gain weight? Well, he argues that there’s good fat and bad fat; there’s sick fat and healthy fat.
When you look at healthy fat, you see an excellent expansion. On the other hand, Sick fat has inflammation, produces fibrosis, and has macrophages, macro meaning large and -phage meaning eats or consume. Macrophages are a group of cells that can be good and help replace injured tissue or can be harmful and involve more inflammation. Healthy fat is very different.
The ominous features of adipose (fat) tissue dysfunction are inflammation, fibrosis, and impaired angiogenesis; angio means vessel, and genesis means to make; that’s impairment of blood vessel development. When you get fibrosis, inflammation, and loss of blood supply to the expanding fat cell, it becomes an anaerobic environment; it loses its vasculature.
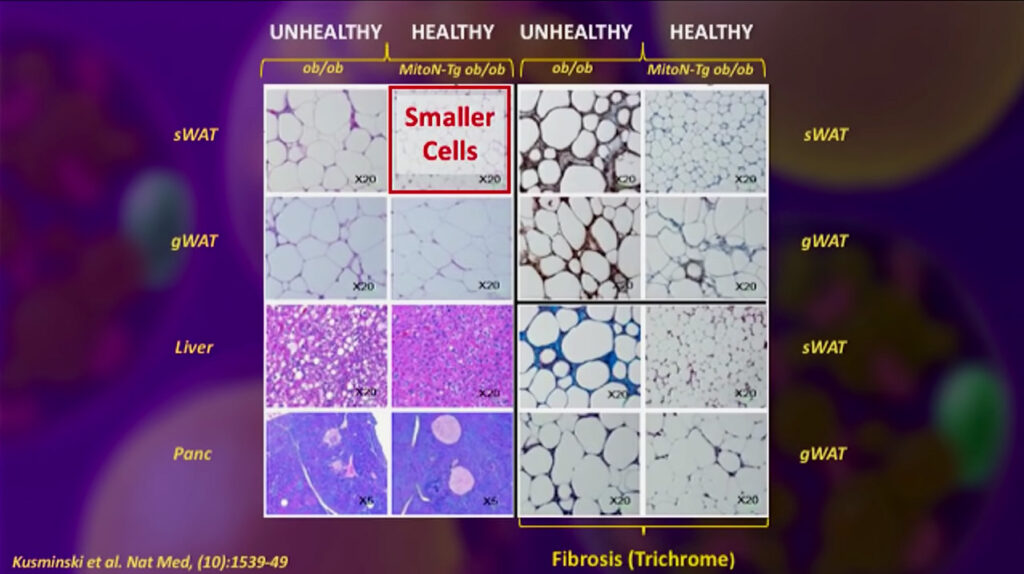
The pictures below give you a microscopic view of what some of this tissue looks like. When you have reduced fibrosis, you have smaller cells; they tend to be healthier cells and have reduced chronic inflammation; this is what you want, more cells, but smaller.
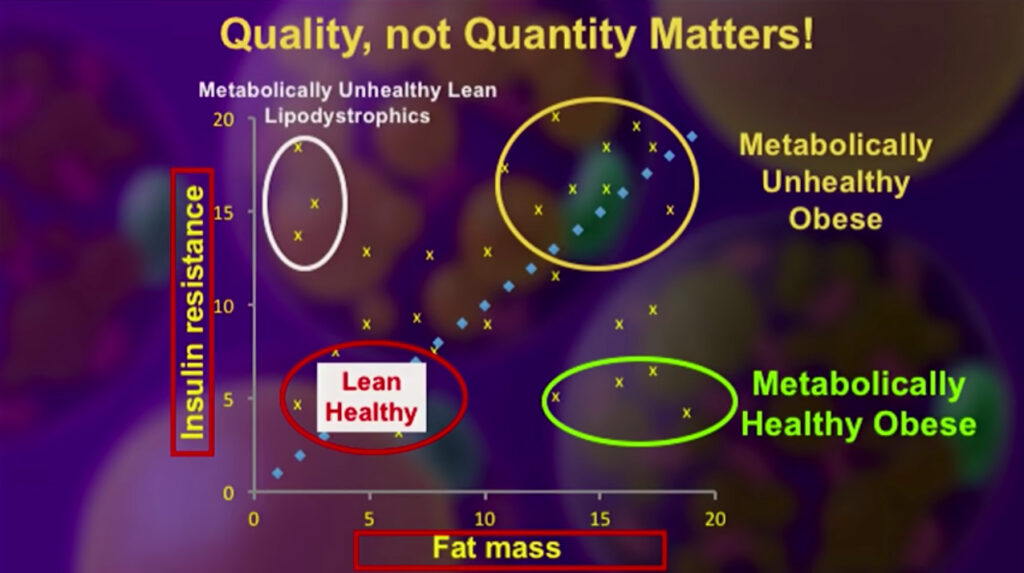
The following chart shows fat mass in the bottom axis, and insulin resistance on the side axis; as you can see, in the upper right-hand corner are the metabolically unhealthy, obese; in the lower left-hand corner are the lean, healthy, in the lower-right corner is the metabolically healthy obese people, and in the upper left hand you see people that have full-blown lipodystrophy. Lipo means fat; dystrophy means misplaced fat; these people are unhealthy but lean, have insulin resistance, and often severe diabetes, yet they’re skinny. They have little to no subcutaneous fat; however, they have fat within the liver and muscles.
There are some different types of fat, brown fat, which is brown, is metabolically healthy; beige fat, metabolically, is a little healthier than white. Brown Adipocytes, Adipo meaning fat, and cytes meaning cells were unknown until a few years ago. One key concept to remember is that adipocytes are not just a simple type of cell.
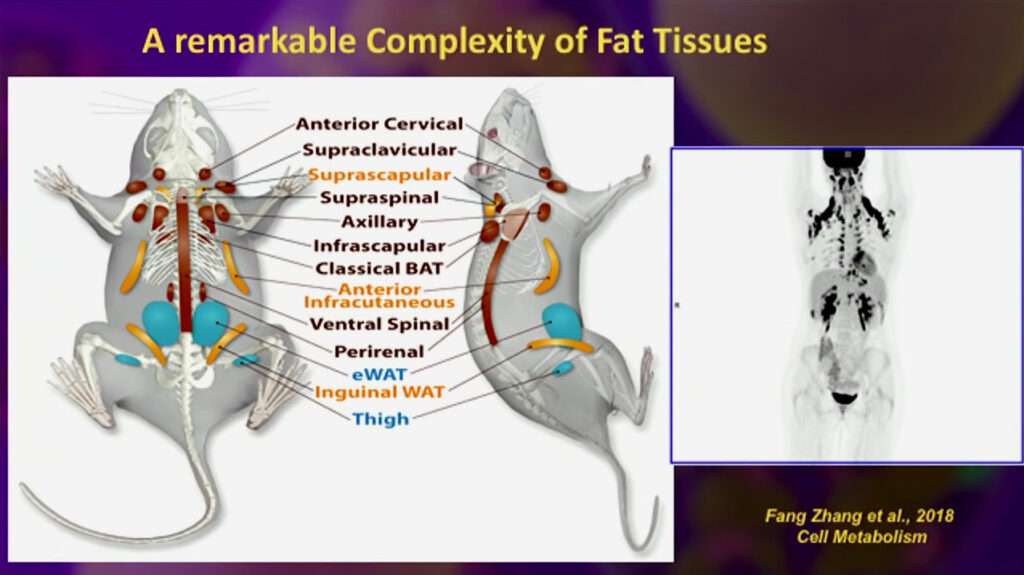
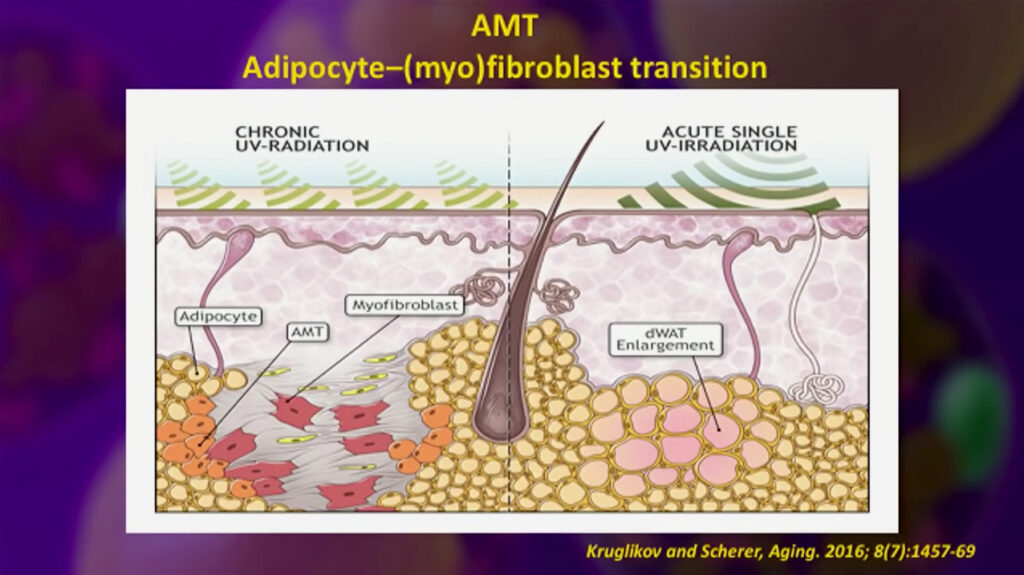
Below you will see a mouse diagram showing the distribution of complex fatty tissues; you will see the colors as well, some brown areas, and some of the beige regions, and in the following image, you can see what’s called a transition from an adipocyte to a myofibroblast, this is important because evidence shows that adipocytes can undergo a transition back into a stem cell.
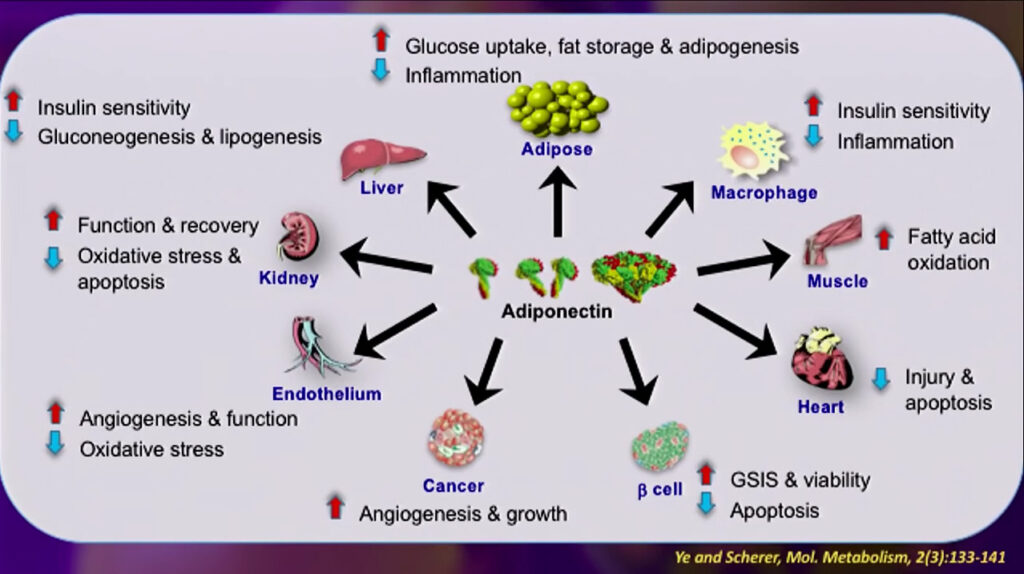
Another fact adipocytes are not inactive cells is that they produce adiponectin, although metabolically unhealthy cells produce low adiponectin. Adiponectin levels In plasma are inversely proportional to the fat mass. Adiponectin levels are excellent integrators of fat tissue and help systemic insulin sensitivity.
Adiponectin has taught us that a fat-derived factor can be anti-apoptotic; apoptosis means cell death; therefore, adiponectin might protect against cell death in our body. It is also pro- angiogenic; it can create blood vessels and decrease plaque formation, inflammation and fibrosis; adiponectin also promotes fat creation and even promotes insulin sensitivity.
Adiponectin has become one of the best biomarkers of existing metabolic, cardiovascular, and diabetes-related diseases.
Lastly, he talks about ceramides; ceramides are another class of fatty acids; with an increase of ceramides, there is more insulin resistance and inflammation; however, sphingosine, an essential compound involved in the cell membrane structure, improves insulin sensitivity and decreases inflammation.
Dr. Scherer showed how decreasing ceramides in fat cells improves insulin sensitivity in fat and the liver, positively affecting diabetes and prediabetes.
It’s more complicated than we thought, but this is a very positive development. It creates opportunities to understand insulin resistance, the evolution of cancers, and how to manage our fat.
If you want to know more, take a look at Dr. Scherer’s vídeo here:
If you found this article helpful and want to start taking steps toward reversing your chronic disease, Dr. Brewer and the PrevMed staff are ready to serve you no matter where you’re located.
To find out more, schedule a consult here: prevmedhealth.com
REFERENCES
- https://science.sciencemag.org/content/355/6330/eaaf5375.full “An adipo-biliary-uridine axis that regulates energy homeostasis Science 17 Mar 2017:” Vol. 355, Issue 6330, eaaf5375
- https://prevmedhealth.com/the-3-biggest-diet-mistakes-theyre-not-food-choices-part-2/
- https://prevmedhealth.com/is-saturated-fat-unhealthy-is-it-a-big-fat-surprise-big-fat-lies-or-just-confusion/
- Dr. Scherer’s UTSW Presidential Lecture, available at: https://youtu.be/zEBfwwpcTzU